Thursday marks the formal end of the federal government’s COVID-19 public health emergency, three years after it was first declared.
The novel coronavirus started a pandemic that killed 1.1 million Americans and sickened millions more. Today, deaths and hospitalizations are at record lows, and much of the public has moved on.
But the virus is still killing hundreds of people a day, and public health experts are cautioning that there could be future surges if it mutates enough to escape vaccines.
The end of the public health emergency is more than a symbolic declaration. The flexibilities it granted touched on almost all aspects of the U.S. health care system, and unwinding it will not be easy.
Significant changes could impact testing and treatment, vaccines, data reporting, and insurance coverage. Here’s what that means for you:
Vaccines and Paxlovid will still be free
The federal government’s administration of COVID-19 vaccines and treatments is not impacted by the end of the public health emergency.
But the Biden administration says it does not have money to purchase new doses. The administration has been coordinating with manufacturers to make sure they have enough on-hand supply of tests, treatments and vaccines to put onto the commercial market when the government involvement ends.
If you have private insurance, the shots will still be free, though the cost will likely be reflected in premiums. Moderna and Pfizer plan to charge at least $110 per dose for their vaccines on the private market.
Treatments like Paxlovid will also come with cost-sharing for people with private insurance.
Even with insurance, patients will likely see costs if they go to an out-of-network provider.
The biggest impact will be on uninsured or underinsured Americans, many of whom have jobs that put them at greater risk of COVID-19 exposure.
The administration’s “Bridge to Access” program would keep a limited supply of vaccines and therapeutics on hand to distribute free through state and local health departments for months after the transition.
The administration also secured limited funding to pay pharmacy chains that will enable them to continue offering free COVID-19 vaccinations and treatments to the uninsured through December 2024.
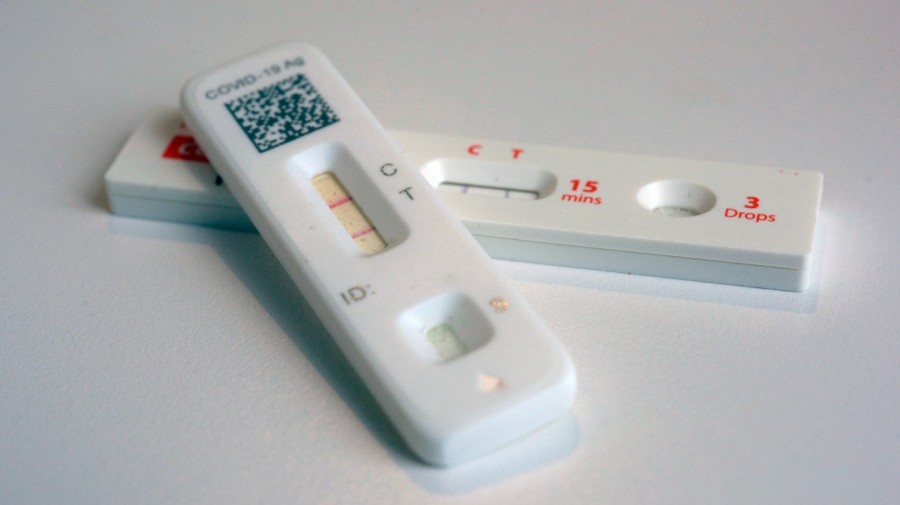
At-home COVID-19 tests won’t be free
If you have private insurance, you’ll probably have to pay full price for an at-home COVID-19 test.
A KFF analysis found that the median cost of an outpatient COVID-19 test was $45 in 2021 for people with large, employer-based health plans.
People who stocked up on tests ahead of time are being advised to check the expiration dates.
For a PCR test administered or ordered by a clinician, people with private insurance will likely face some kind of cost-sharing, either through a copay, deductible or coinsurance. Plans may also enforce quantity limits and prior authorization requirements.
People with traditional Medicare can continue to receive COVID-19 PCR and antigen tests with no cost-sharing when the lab tests are ordered by a physician or certain other health care providers.
You won’t see daily case numbers anymore
The federal government loses a lot of the power it had to mandate certain data reporting.
The Department of Health and Human Services will stop being able to accurately track the number of new infections because labs won’t be required to report test results. States will also no longer be required to report comprehensive data.
Outside the public health emergency, individual states decide what they want to report to the federal government and how often. Some states will also lose their legal authority to collect case data.
As a result, the Centers for Disease Control and Prevention (CDC) will stop posting a national count of new infections, transmission levels and community levels.
Instead, COVID-19–associated hospital admission levels will be the primary indicator of trends to help guide community and personal decisions, the agency said.
“We have the right data for this phase of COVID-19. Though our data going forward will be different, they will continue to provide timely insights for CDC, for local health officials, as well as for the public to understand COVID-19 dynamics at the community level,” CDC Principal Deputy Director Nirav Shah said in a recent briefing.
Telehealth rules have been extended
The public health emergency declaration included major changes related to telehealth, as homebound patients and providers still needed to connect. As a result, requirements were waived so patients could more easily connect by phone or computer to a provider and get prescriptions from a specialist to treat conditions like ADHD or opioid use disorder.
The big changes won’t happen right away, because Congress extended the vast majority of current Medicare telehealth flexibilities through the end of 2024 as part of last year’s government spending bill.
For example, Medicare patients will continue to receive mental health care, as well as some physical services via telehealth.
This week, the Drug Enforcement Administration and the Substance Abuse and Mental Health Services Administration said they will delay the end of the pandemic rules that let doctors prescribe controlled substances using telehealth.
The agencies had previously planned to roll back the flexibility and reinstate in-person visit requirements for drugs including Adderall, testosterone for hormone replacement therapy, and buprenorphine.












{kind=link}